
Patient Stories
 URGO Medical is proud to announce that its “Tissue Viability & Wound Care Practice” education program has been re-endorsed by the Australian College of Nursing through until 2024.
URGO Medical is proud to announce that its “Tissue Viability & Wound Care Practice” education program has been re-endorsed by the Australian College of Nursing through until 2024.This Training and Workshop is endorsed by ACN according to the Continuing Professional Development (CPD) Endorsed Course Standards. It has been allocated 14CPD hours according to the Nursing and Midwifery Board of Australia – Continuing Professional Development Standard.
Tissue Viability is explained as preventing insults to the skin and underlying tissues and facilitating healing in wounds where a complication has prevented the normal healing process. It is an umbrella term, which, when used correctly, refers to the prevention and management of tissue damage which may include both acute and chronic wounds, and the provision of the appropriate environment for healing by both direct and indirect methods together with the prevention of skin breakdown.
This 2-day program is intended as a platform where basic to intermediate training is provided for those health care practitioners who are interested in acquiring further knowledge in the area of wound management. Eight modules introduce the participant to the fundamentals of the Integumentary System, the causes and assessment of wounds, how wounds heal and the holistic treatment of alternative wound healing etiologies using an evidence based approach. The aim of the program is to enhance clinicians practice when dealing with management of and prevention of tissue complications. The workshop includes didactic information via PowerPoint, interactive sessions in the form of group activities, knowledge checks and scenarios or case studies, plus hands-on learning (where applicable).
The URGO Education & Training Alliance has been established with the sole purpose of providing unbiased evidence based education to clinicians. The Chairman and main educational sessions facilitator, Emilio Galea, has a long history in the field of wound management and tissue viability with local individual facilitators Cassandra Hough and Tanya O’Hara – both clinical specialists with URGO Medical Australia.
For a more detailed outline of the modules please do not hesitate to discuss with your local URGO representative. This may be an opportunity to support ongoing education and development of up and coming wound care nurses, assist with the development of wound care champions or up skill team members. The facilitators can also tailor the program to meet the needs of your team with days and times negotiable.
For more information please contact us or email: enquiries@au.urgo.com
Delayed or inaccurate diagnosis can cause complications and extended treatment durations.
30% of wounds lack differential diagnosis7
Only 22% of patients had an ABPI documented7
42% of wounds remain unhealed after 6 months7
Chronic venous hypertension >70%
Poor arterial supply10-15%
Mixed arterial and venous origin 15%
(i.e. obesity, malnutrition, diabetes, inflammatory conditions), lifestyle and increased longevity)
The priority for leg ulcer patients is to reduce healing time to get back to their normal life.
To reverse Venous Hypertension
To remove local factors that impair healing
Why do leg ulcers take so long to heal?
Beyond the underlying etiology of leg ulcers, one key local factor significantly impairs wound healing from the beginning:
A prolonged inflammatory phase with increased levels of Matrix Metalloproteinases (MMPs)10 which are present
from the beginning of the wound and destroy essential extracellular matrix (ECM) components.
Interactive dressings that address local barriers to healing can reduce healing time for leg ulcer patients
In addition to the etiologic treatment such as off-loading and compression, a local treatment is needed to act on this factor.
Reduction of excess Matrix Metalloproteinases (MMPs):NOSF has been shown to reduce healing times.10
Since MMPs are the main enzymes implicated in the extracellular matrix (ECM) degradation, their reduction results in a reduction of proteolytic destruction of essential ECM components.
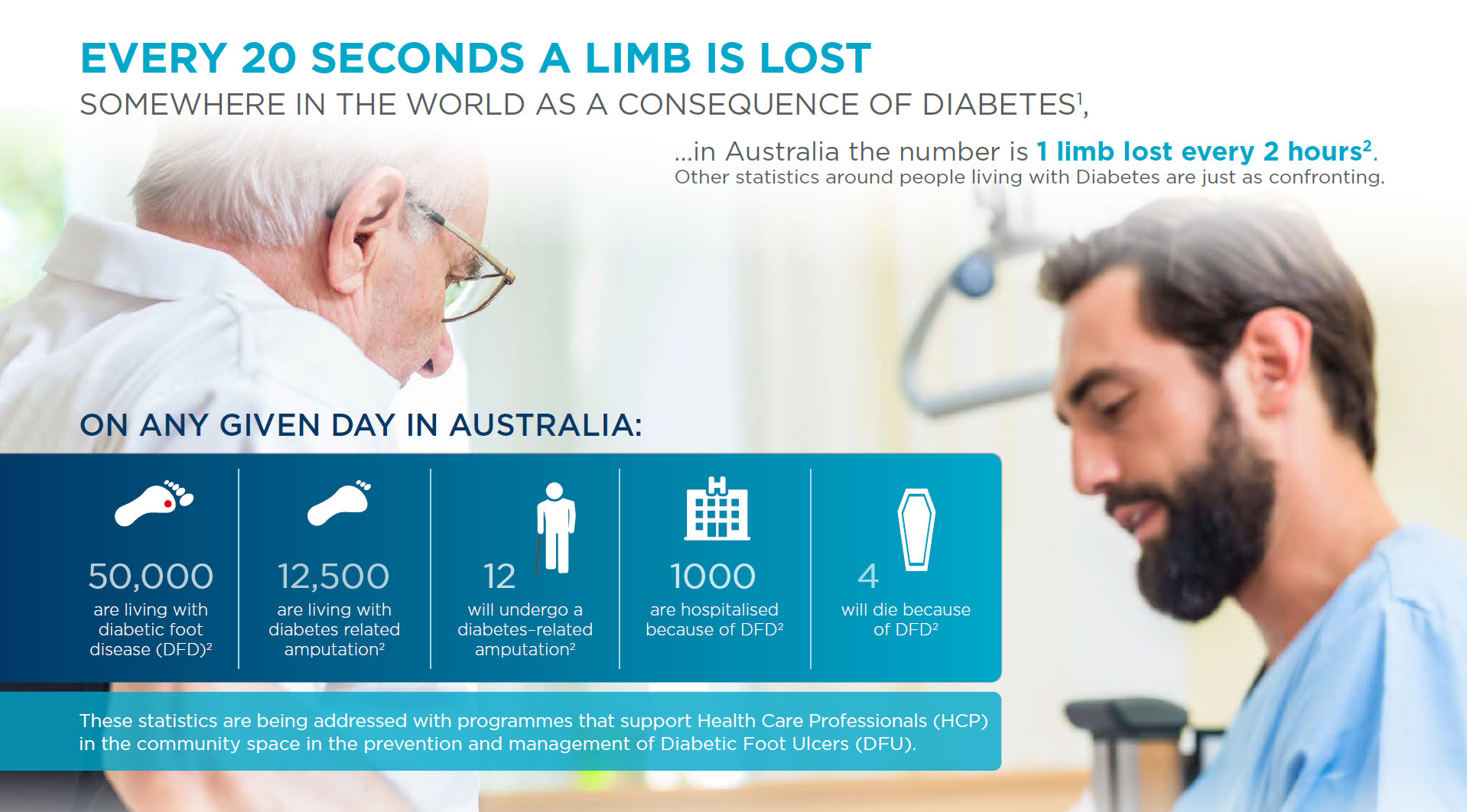
Diabetic foot ulcers (DFUs)are one of the major complications of diabetes. Between 19 and 34% of all diabetics will develop a foot ulcer at some point in their lives3 DFUs can lead to complications such as an infection requiring hospitalisation, or in the worst cases, amputation. After amputation, patient life expectancy does not exceed 5 years in almost 70% of cases4.
The prevention of DFUs requires a partnership of those people living with Diabetes and their HCP. This partnership should be underpinned with daily foot checks undertaken by the patient, reinforced by regularly scheduled visits to their HCP for a more detailed check that should, at a minimum include a check for Loss of Protective Sensation (LOPS) due to neuropathy and Peripheral Artery Disease (PAD). Both of these are major risk factors in the development of DFUs.
To assist in the rating of patient’s risk of developing a DFU URGO Medical Australia have provided Fact Sheets for both General Practitioners and their patients, now available in Medical Director and Best Practice, on diagnosis.
This Fact Sheet also provides GPs with a link to the Australian Save Feet/Save Lives website where you can find more information on the prevention of DFUs. A non-HCP version of the site is also available for patients to learn more about Diabetes and preventative care of their feet.

With the best of efforts, a large number of DFUs still occur. This is when closing wounds earlier reduces the risk of amputation 5,6. There are steps that can be taken by front line healthcare practitioners to better managing a DFU.
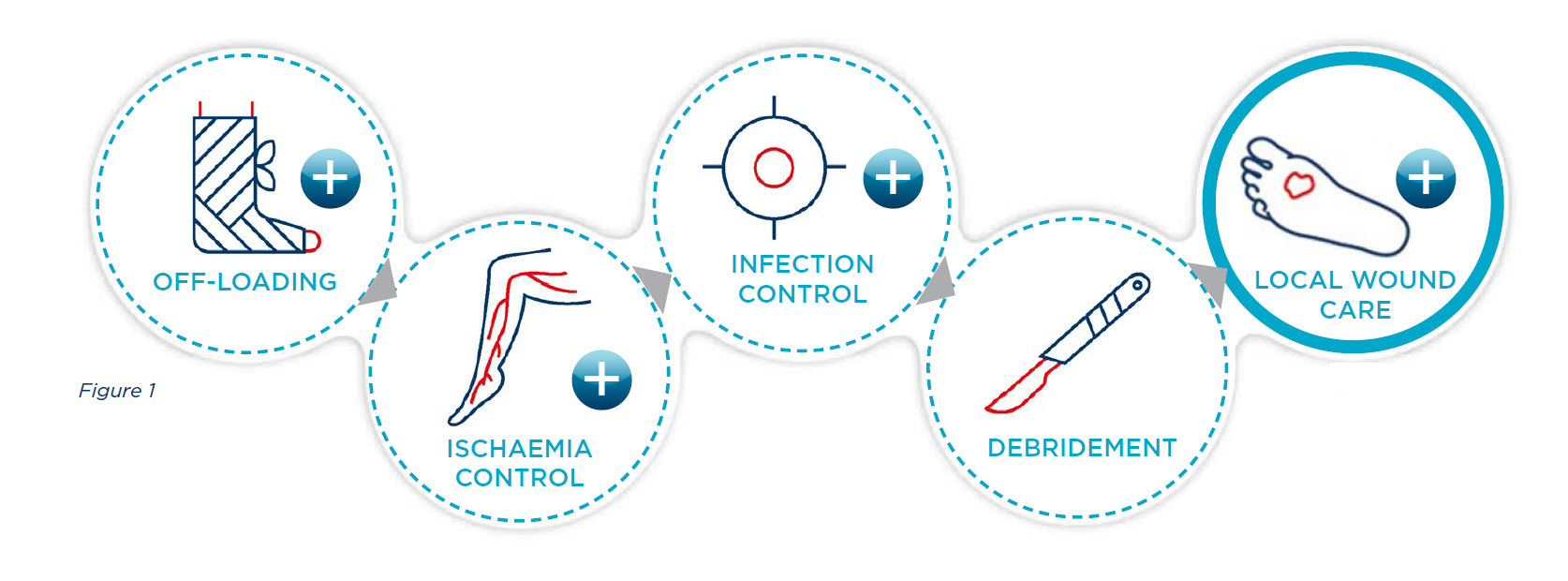
UNDERSTAND THE STANDARD OF CARE FOR DIABETIC FOOT ULCERATION. DFU treatment is complex and requires a multidisciplinary approach. This is the recommended standard of care that needs to be put in place by a multidisciplinary team in a specialised setting5,6 (also see figure 1)

Several factors can cause a wound, compromise its healing, or even cause an acute wound to become a chronic wound, with all the risks of complications that brings, including the risk of recurrence. Below are some of the risk factors usually present:
